In the world of clinical podiatry, big toe pain is often dismissed as a singular symptom. But for the patient, the experience is vastly different depending on the underlying pathology. Two of the most commonly confused foot injuries are Hallux Rigidus and Turf Toe. While both center on the first metatarsophalangeal (MTP) joint, they represent a fundamental conflict between traumatic failure and structural degeneration.
The 2026 Diagnostic: The core difference between Hallux Rigidus and Turf Toe is onset and mechanism. Turf Toe is an acute soft-tissue “snap” caused by sudden hyperextension during activity. Hallux Rigidus is a chronic, progressive “grind” where cartilage wear leads to a physical bone-on-bone blockade.

Anatomy of Failure: Beyond Big Toe Pain
Understanding the difference between these two conditions requires looking beneath the skin at how the MTP joint fails under stress.
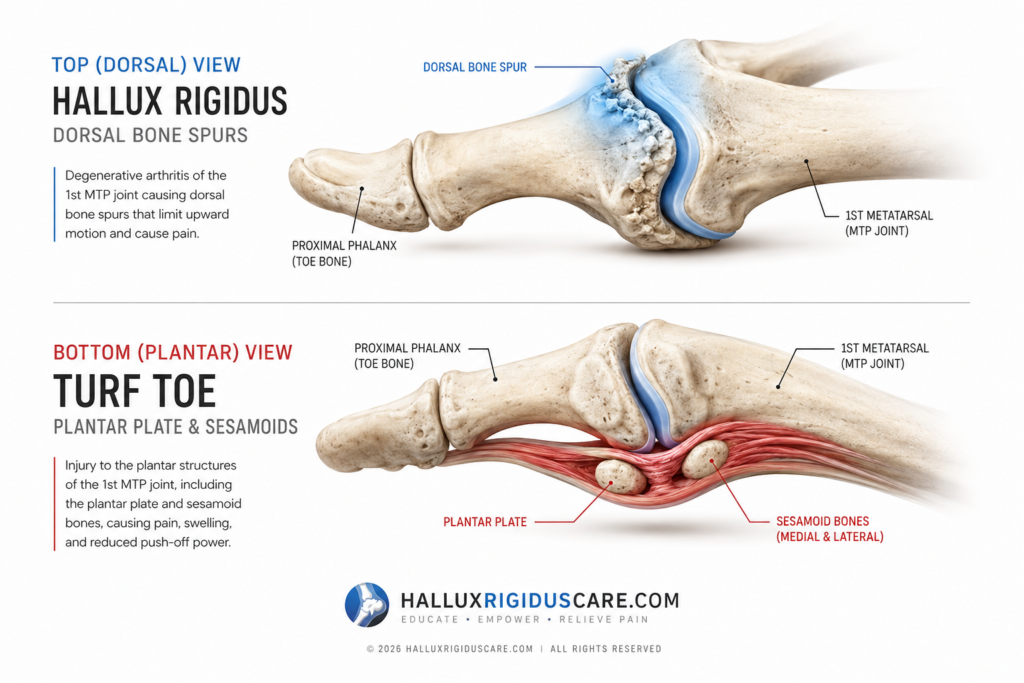
Turf Toe: The Soft Tissue Snap
Turf toe is a sprain of the ligaments and soft tissue surrounding the first MTP joint. It is most common among athletes who play on artificial surfaces, where high friction and firm ground cause the big toe to be forced into hyperextension.
- The Mechanism: The “Plantar Plate”—a thick fibrous structure under the joint, is stretched or torn.
- The Grading: A Grade 1 injury is a minor stretch, while a Grade 3 is a complete tear that can lead to joint instability or even dislocation.
- The Sensation: Often described as an immediate “pop” or sharp “snap” followed by rapid swelling on the bottom (plantar) side of the toe.
Hallux Rigidus: The Structural Block
Unlike a sprain, Hallux Rigidus is a form of degenerative arthritis. It is a “wear and tear” condition where the articular cartilage that allows smooth movement is eroded.
- The Mechanism: As cartilage vanishes, the body attempts to stabilize the joint by growing bone spurs (dorsal osteophytes) on the top of the joint.
- The Blockade: These bone spurs act like a physical doorstop. When you attempt to walk, your toe tries to bend upward, but the bone spurs on top jam together, stopping the motion entirely.
The “Gateway” Warning: Clinical research indicates a critical link: repeated or severe Turf Toe injuries in younger athletes can shred the joint’s cartilage. It acts as a “gateway” that fast-tracks the development of Hallux Rigidus later in life.
The “Limp Compensation Loop”: Referred Pain
One of the most significant clinical gaps in big toe education is the failure to address the kinetic chain. Big toe joint failure is rarely an isolated incident; rather, it is a structural chain reaction that often manifests as pain elsewhere in the body.
The Mechanics of Gait Sabotage
When the big toe joint is locked by Hallux Rigidus or unstable from Turf Toe, the body instinctively alters its gait to avoid pressure on the MTP joint. This is known as the Limp Compensation Loop.
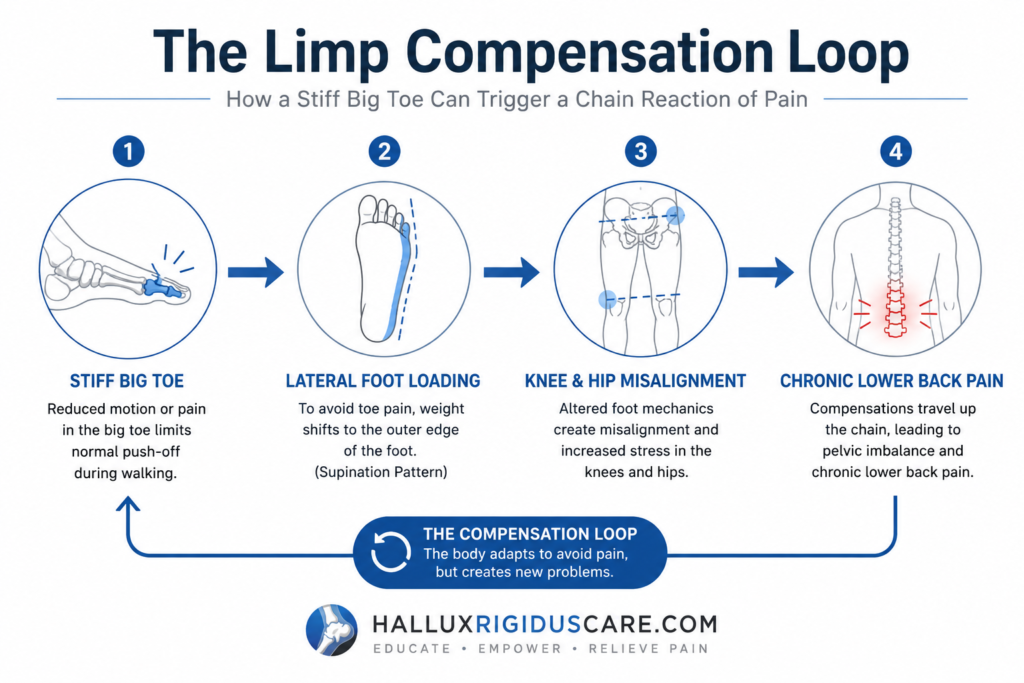
- Lateral Loading: Patients often walk on the outer edge of the foot (supination) to bypass the big toe during the “push-off” phase.
- The Hip-to-Back Chain: This lateral shift forces the hip and knee into non-neutral positions, leading to premature joint wear.
- Referred Pain: Consequently, persistent gait compensation is a primary driver of lower back pain and hip bursitis in 2026. Treating the toe often resolves these “mysterious” chronic issues.
2026 Treatment Standards: Mechanical Offloading
In 2026, recovery protocols have shifted from passive “rest” to active mechanical offloading. This approach keeps you mobile while protecting the injured structures.
Turf Toe: Taping and Stabilization
For acute ligament tears, the priority is preventing further hyperextension.
- Dynamic Taping: Using specialized “Figure-8” taping to pull the toe into a slightly downward (plantarflexed) position.
- Stability Inserts: A full-length carbon fiber plate is the gold standard. It prevents the shoe from flexing, which protects the plantar plate during sports.
Hallux Rigidus: The Rocker-Bottom Shift
Since Hallux Rigidus involves a structural blockage (the bone spur), the shoe must do the work the joint no longer can.
- Rocker-Bottom Geometry: Shoes with a curved sole (like HOKA or Brooks) allow the foot to “roll” forward without the big toe needing to bend.
- Morton’s Extension: This specialized orthotic adds rigidity specifically under the first MTP joint, effectively stopping the “grind” of bone spurs.

Clinical Interventions: When to See a Surgeon
If mechanical offloading fails to manage the pain, advanced 2026 interventions are necessary to restore quality of life.
- Weight-Bearing X-Rays: It is essential to get weight-bearing radiographic imaging, as traditional ‘lying down’ X-rays often miss the mechanical joint jamming that occurs under the pressure of a full step
- Diagnostic Injections: Dr. Sarah Jenkins often uses a temporary numbing agent inside the joint. If the pain vanishes, the issue is intra-articular (Hallux Rigidus); if it persists, it is likely soft-tissue (Turf Toe).
- Cheilectomy: A popular 2026 surgical “cleanup” procedure in which dorsal bone spurs are removed to restore motion without the need for a full joint fusion.
The Road to Recovery: Protocol and Timeline
Recovery is not a one-size-fits-all process. The timeline is dictated by whether you are managing a chronic degeneration (Hallux Rigidus) or healing an acute trauma (Turf Toe).
Healing Turf Toe (The Regenerative Path)
- Grade 1 (1–2 Weeks): Immediate rest, compression, and a stiff-soled shoe typically allow the ligaments to tighten back up.
- Grade 2 (3–6 Weeks): This often requires a walking boot or a “non-weight-bearing” period to allow partial tears to bridge.
- Grade 3 (2–4 Months): Significant tears require intensive physical therapy and, in some 2026 protocols, regenerative injections to restore the integrity of the Plantar Plate.
Managing Hallux Rigidus (The Maintenance Path)
- Initial Flare-Up (2–3 Weeks): Using NSAIDs and “Contrast Baths” to calm the inflammation around the dorsal bone spurs.
- Long-Term Strategy: Since cartilage does not regrow, recovery is measured by the absence of pain during activity. This is achieved through permanent footwear modifications and maintaining joint mobility through “distraction” exercises.
Long-Term Prognosis: Life After Big Toe Injury
A common concern in 2026 is whether these injuries end an active lifestyle. The answer depends on mechanical compliance.
- The Athlete’s Outlook: With modern carbon fiber stabilization, most athletes return to 100% performance following Turf Toe. However, they must remain vigilant; a “healed” Turf Toe joint is more susceptible to future stiffness.
- The Hallux Rigidus Outlook: While Hallux Rigidus is progressive, it is highly manageable. Many patients avoid surgery for decades by strictly adhering to Rocker-Bottom footwear and avoiding “barefoot” stressors like certain yoga poses or minimalist running.
Conclusion: Protecting Your Foundation
Your big toe is the anchor of your entire kinetic chain. As this guide has shown, the path to recovery depends entirely on determining whether you are dealing with an acute ligament snap or a chronic mechanical grind. Ignoring these nuances doesn’t just lead to a stiff toe; it invites a structural chain reaction known as the Limp Compensation Loop.