If you are researching whether hallux rigidus can be reversed, you are likely at a crossroads. Perhaps you’ve just seen a “bone spur” on an X-ray for the first time, or maybe the sharp, grinding pain at the base of your big toe has finally started to dictate which shoes you can wear. As a Senior Orthopedic Podiatrist, the most frequent question I receive in my consulting room is:
The $10,000 Question
“Dr. Reynolds, can we fix this without surgery?”
The Short Answer: Biologically, no. Mechanically, yes.
The honest answer, the one backed by clinical evidence rather than marketing fluff, is nuanced. To provide a definitive answer, we must first distinguish between Radiographic Reversal (changing the physical structure of the bone) and Symptomatic Reversal (eliminating pain and restoring function). One is a biological impossibility in 2026; the other is a goal we achieve for our patients every single day.
Wait! Did You Know?
Most people think “Bone Spurs” are the cause of pain. They aren’t! The pain actually comes from your body trying to heal a joint it can no longer lubricate. The spur is just a symptom!
Biological Reality: Why Big Toe Cartilage Cannot Structurally Regrow
To understand why hallux rigidus cannot be biologically reversed, we have to look at the unique, almost tragic nature of hyaline cartilage. This is the slippery, pearlescent coating that caps the end of your metatarsal bone in the first MTP joint. It is the most efficient friction-reducing substance known to man, smoother than ice on ice.
However, cartilage has a fatal flaw: it is avascular (no blood supply) and aneural (no nerves). Unlike your skin, which heals with a scab, cartilage has no internal ‘repair crew’ because it lacks a direct blood supply, a biological limitation well-documented by the National Institutes of Health. When you lose cartilage due to the wear-and-tear of hallux rigidus, the body does not replace it with new, healthy hyaline cartilage. Instead, if it repairs at all, it produces fibrocartilage, a tough, scarred version of tissue that lacks the shock-absorbing properties of the original.
In this sense, hallux rigidus cannot be “cured” or “reversed” in a structural way. Once the joint space has narrowed and the protective coating is gone, mainstream medicine cannot currently grow it back. No amount of collagen supplements, turmeric, or “natural” remedies can regenerate the microscopic architecture of a degraded MTP joint.
The “Structural Rubicon”: Identifying the Point of No Return
In my practice, I guide patients through a concept I call the Structural Rubicon. This is the invisible line that separates a functional problem from a structural disease.
Before you cross this line, you are likely dealing with Hallux Rigidus vs. Hallux Limitus. At the “Limitus” stage, your joint is physically healthy, but its movement is blocked by a mechanical jam, often caused by a tight calf muscle or a hypermobile foot type. At this stage, reversal is 100% possible. By using aggressive physical therapy and custom orthotics, we can “unlock” the joint and restore a full 60° range of motion.
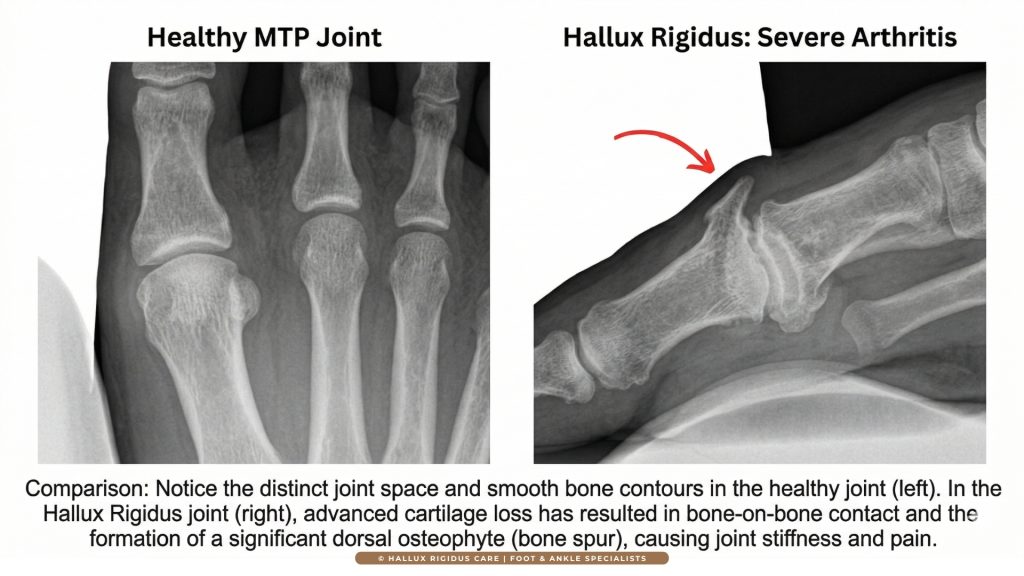
However, once you cross the Rubicon into true Hallux Rigidus, the environment changes. The friction from that mechanical jam begins to wear away the cartilage physically. To protect itself, your bone reacts by growing “Osteophytes”—jagged bone spurs on the top of the joint. These spurs act like a physical doorstop. No amount of stretching can “reverse” a solid wall of bone.
Have you noticed this yet?
“Do you find yourself rolling your foot to the outside edge when you walk to avoid the big toe pain? This is called ‘Supination Escape,’ and it’s the first sign you’ve crossed the Rubicon. Are you also feeling new pain in your ankle or knee?”
Symptomatic Reversal: The 2026 Goal
If a “cure” is a biological impossibility, why do I tell my patients that a pain-free life is still achievable? Because Symptomatic Reversal defines clinical success. You can have a Grade 2 arthritis finding on an X-ray and experience zero pain during a 5-mile walk. This is achieved by “deactivating” the arthritis. By changing the physics of how your foot hits the ground, we can prevent the joint from reaching its painful “jamming point.” If the inflammation is gone, the “need” for a biological cure disappears. This is the “Honest Answer” promised in this guide: We don’t fix the X-ray; we fix your life.
Are you feeling “The Grind”?
Have you noticed a sharp, burning sensation when you try to “push off” while walking uphill? That is the Windlass Mechanism failing. You aren’t just tired; your foot is physically shouting for a mechanical change.
The Physics of the Big Toe: Why It Hurts
The big toe is the “engine” of your gait. During the “toe-off” phase of walking, this small joint bears approximately 1.2 to 1.5 times your total body weight. If you weigh 180 lbs, that tiny joint is absorbing nearly 270 lbs of force with every single step. If you run, that force jumps to 3x or 4x your body weight.
When your cartilage is thin, that pressure is no longer distributed; it is concentrated on raw bone. Reversal, in a practical sense, means offloading that pressure. If we can reduce that 270 lbs of force down to a manageable load through mechanical interventions, we have effectively “reversed” the disease’s impact on your daily life.
Hallux Rigidus Stages 0-4: Identifying Your “Point of No Return”
In clinical practice, the most dangerous moment for a patient isn’t the diagnosis of hallux rigidus; it is the misunderstanding of their current stage. Patients often come to me saying, “My toe is stiff,” but there is a world of difference between a toe that is physically blocked and a toe that is biologically decayed. To answer whether your condition can be “reversed,” we must use the Coughlin-Shurnas Grading System, the gold standard in orthopedic staging. This is how we determine if we are fighting a mechanical “jam” or a structural “lockdown.”
Understanding your specific grade is the only way to establish a realistic treatment timeline. If you treat a Grade 3 joint with Grade 0 protocols, you will fail. Conversely, if you jump to surgery for a Grade 1 joint, you may be over-treating a problem that could have been managed mechanically.
Grade 0 & 1: The “Functional” Stage (The Only True Reversal Window)
At Grade 0 and Grade 1, the joint structure remains largely intact. If we were to look at your weight-bearing X-ray, the joint space would appear wide, and the bone surfaces would be smooth. However, when you walk, the toe “jams.”
This is what I call Functional Hallux Limitus. The “reversal” here is highly achievable because the problem is not the bone; it is the tension. Usually, an underlying biomechanical issue, such as a tight Achilles tendon or a hypermobile first ray, is forcing the joint to “lock” prematurely during your stride. In this stage, you don’t need a surgeon; you need a gait overhaul. By using aggressive physical therapy to restore the “Windlass Mechanism” and adopting custom orthotics, we can often “reset” the joint’s timing. Data shows that early intervention at Grade 1 can delay the need for surgery by 10 to 15 years, and in many cases, indefinitely.
Grade 2: The “Intermediate” Battleground
Grade 2 is where the “Honest Answer” becomes more complex. At this stage, you have likely developed a Dorsal Osteophyte, the signature bone spur on the top of the joint. You might feel a hard “bump” that makes wearing certain footwear painful. On an X-ray, I will begin to see the joint space narrowing, usually by about 25% to 50%.
Can Grade 2 be reversed? Biologically, no. That bone spur is a permanent structural change; it will not dissolve with diet or exercise. However, Symptomatically, yes. At Grade 2, the joint usually still has enough healthy “central” cartilage to function without pain, provided we stop the “end-range” grinding. This is the stage where your choice of footwear becomes your primary medicine. By switching to the Best Walking Shoes for Hallux Rigidus, you prevent the toe from hitting that bone spur “wall.” You are not “curing” the spur, but you are effectively “reversing” the pain cycle by bypassing the damaged area.
Grade 3 & 4: The “Structural” Lockdown
Once a patient hits Grade 3, the cartilage loss is no longer localized; it is widespread. The protective “gap” between your bones has narrowed by more than 50%, and pain occurs not just when pushing off, but even when resting. Grade 4 is the final stage, where the joint has nearly zero motion, and the pain is constant.
At this point, “reversal” through shoes or injections is no longer a realistic clinical goal. My role as a surgeon shifts from Joint Preservation to Pain Elimination. While we cannot reverse a Grade 4 joint back to a Grade 0, we can use surgical interventions like Arthrodesis (Fusion) to “reverse” the patient’s lifestyle from sedentary back to active. It is a paradox of podiatry: sometimes, removing the motion entirely is the only way to restore the patient’s ability to move.
The “Rubicon” Moment: How to Tell if You’ve Crossed It
The easiest way to tell if your condition has moved from “reversible” to “permanent” is the Mid-Range Pain Test.
- Sitting Test: If your toe only hurts when you manually push it to its extreme end-range (bending it back toward your shin), you are likely still in the preservation window.
- Walking Test: If it hurts the moment you begin to move the toe during a step, the cartilage loss has likely become global.
An X-ray is a map, but your symptoms are the compass.
I have seen Grade 3 patients who are pain-free because they switched to stiff-soled shoes, and Grade 1 patients crippled by pain because they refuse to give up flexible sneakers. Your grading is not your destiny; it is a baseline that we can manage mechanically.
Dr. Reynolds’ Staging Recognition Matrix
Mechanical Reversal: How Rocker-Bottom Shoes “Bypass” Joint Pain
The Windlass Mechanism: Why Your Shoes Are Failing You
To understand why specific footwear is required, you must understand the Windlass Mechanism. In a healthy foot, as you push off the ground, your big toe bends upward (dorsiflexion). This action pulls the plantar fascia tight, arching the foot and turning it into a rigid lever for propulsion.
Are you suffering every morning?
If your first 10 steps of the day feel like walking on glass, your joint is in Active Inflammation. Let’s look at the mechanical “bypass” that stops this immediately.
In a patient with hallux rigidus, this mechanism becomes a source of destruction. Because the joint is stiff or blocked by a bone spur, your body still tries to force that bend. This results in “bone-on-bone” grinding that accelerates cartilage loss. Most modern athletic shoes are designed to be “flexible,” which is exactly what a rigid toe cannot handle. If your shoe bends where your toe cannot, you are essentially sandpapering your remaining cartilage with every step.
The Rocker-Bottom Revolution: A Mechanical Bypass
The single most effective tool in our “reversal” toolkit is the rocker-bottom sole. I tell my patients to think of a rocker-bottom shoe as a “mechanical bypass.” Instead of your MTP joint bending 60 degrees to move you forward, the curved sole of the shoe performs the “roll” for you.
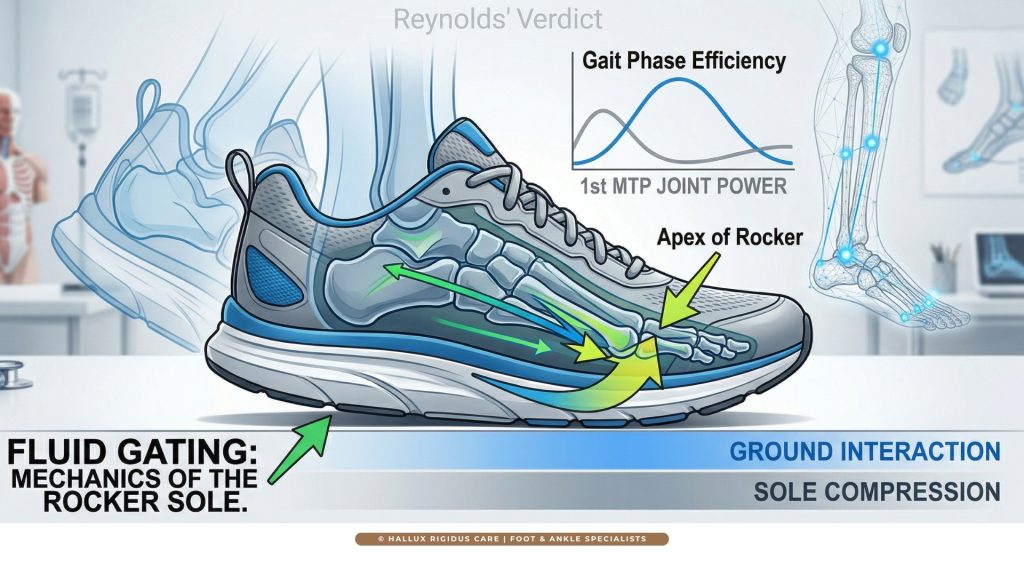
When selecting the Best Walking Shoes for Hallux Rigidus, we look for a specific “apex” point in the rocker. A forefoot rocker reduces the energy required for toe-off by up to 35%, effectively “silencing” the inflammatory response in the joint. By using these shoes, you aren’t just managing pain; you are physically preventing the bone-on-bone impingement that leads to Grade 3 and 4 disease.
Morton’s Extension: The “Internal Brace”
While a rocker-bottom shoe handles the outside, a Morton’s Extension orthotic handles the inside. This is a rigid carbon-fiber or plastic plate that sits directly under the big toe. Many patients are surprised when I prescribe a “stiff” insert for a “stiff” toe, but the logic is sound: if the joint cannot move safely, we must stop it from moving entirely.
Clinical studies indicate that a Morton’s Extension can reduce MTP joint dorsiflexion by 45–50%. When combined with a stiff-soled shoe, the pressure on the dorsal osteophyte (the “bump”) drops significantly.
The Physics of Offloading (Shoe Features)
Rocker-Bottom Sole
The Physics: Mimics joint dorsiflexion. It performs the “roll” for your foot so the big toe doesn’t have to bend.
Morton’s Extension
The Physics: A rigid carbon-fiber plate that sits under the toe to prevent movement entirely, acting as an internal brace.
Deep Toe Box
The Physics: Increases lateral and vertical space to eliminate friction on dorsal bone spurs (the “bump”).
The “Gait Compensation” Warning
If you do not implement these mechanical changes, your brain will find its own way to “reverse” the pain: the Supination Escape. You will subconsciously roll your foot outward to walk on your pinky toe side. While this saves the big toe, it destroys the kinetic chain.
As a surgeon, I frequently see patients who ignore their hallux rigidus only to end up with chronic ankle instability, lateral knee pain, or even lower back issues. We will dive deeper into this “Domino Effect” in Section 5, but for now, understand that mechanical reversal is about protecting your entire body, not just your toe.
Actionable Advice for 2026: The Stiff-Sole Policy
If you are currently at Grade 1 or 2, your goal is “stiffness.” You want a shoe that you cannot bend with your hands.
Try the “30-Second Shoe Audit”
Take the shoe you are wearing right now. Try to fold it in half at the middle.
The Result: If it bends easily, it’s acting like sandpaper on your joint. If it’s rigid like a plank, you’re on the path to Symptomatic Reversal.
If the shoe folds in half, it is a liability. By adopting a “Stiff-Sole Policy” and utilizing custom orthotics, you are performing the most effective non-surgical intervention available in modern podiatry. You are effectively “freezing” the arthritic process.
The Biological “Wildcards” – PRP, Stem Cells, and 2026 Emerging Meds
As we move into the realm of injections and “regenerative” medicine, we enter the most misunderstood territory of hallux rigidus treatment. In 2026, the internet is flooded with claims of “natural cures” that promise to regrow your cartilage overnight. As a clinician, I must be blunt: there is a massive gap between clinical marketing and clinical evidence. If your goal is to “reverse” the damage through a needle, you need to understand what these substances actually do inside the joint. We are not “growing” new parts; we are optimizing the biological environment to reduce the “fire” of inflammation.
The “Regenerative” Myth vs. Anti-Inflammatory Reality
The term “Regeneration” is often a misnomer in orthopedic medicine. When we talk about PRP (Platelet-Rich Plasma) or Stem Cell Therapy, we aren’t talking about building a new joint. Instead, we are using highly concentrated growth factors to modulate the immune response.
For a patient with Grade 1 or 2 hallux rigidus, the pain isn’t just from the bone spur; it is from synovitis—the inflammation of the joint lining. Injections can effectively “quiet” this synovitis. However, if you have Grade 3 bone-on-bone arthritis, an injection is like throwing a cup of water on a forest fire. It might provide temporary relief, but it cannot “reverse” the structural collapse.
PRP (Platelet-Rich Plasma): Is it Worth the Hype?
PRP has become a staple in 2026 sports medicine. By spinning your own blood to concentrate platelets, we create a “healing cocktail” that can be injected into the MTP joint.
- The Success Rate: For early-stage hallux rigidus, studies show a 60–70% improvement in pain scores for up to 6–9 months.
- The Caveat: PRP does not remove bone spurs. It is best used as a “bridge” to help you tolerate the physical therapy and mechanical changes discussed in Section 3. If you get PRP but continue to wear flexible, unsupportive shoes, you are wasting your money.
Hyaluronic Acid: The “Grease Job”
Often called “viscosupplementation,” Hyaluronic Acid (HA) is a gel-like substance that mimics the natural fluid in your joints. Think of this as a “grease job” for a rusty hinge. While the evidence for HA in the big toe is less robust than in the knee, many of my patients with Grade 2 disease find it provides a “smoother” sensation during walking.
Stem Cells: The 2026 Frontier
I am frequently asked about stem cell injections. While the science of mesenchymal stem cells is advancing, as of 2026, there is no standardized evidence that these injections can reliably regrow articular hyaline cartilage in the human big toe. Most “stem cell” clinics are actually using bone marrow aspirate or umbilical cord tissue. These may have potent anti-inflammatory effects, but calling them a “cure” is scientifically dishonest. In my practice, I classify these as “Experimental Salvage Therapies,” options to try only when everything else has failed, but you aren’t ready for a 1st MTP fusion.
The 2026 Injection Matrix
Corticosteroids
Target: Acute Inflammation
PRP (Platelets)
Target: Grade 1-2 Maintenance
Hyaluronic Acid
Target: Joint Lubrication
The “Natural Cure” Scams
You will see advertisements for “miracle” supplements like high-dose glucosamine or “special” copper-infused socks. Let me save you the time: There is no natural supplement that can remove a dorsal osteophyte. While an anti-inflammatory diet (rich in Omega-3s and low in refined sugars) can help manage the systemic “volume” of your pain, it is a supportive tool, not a reversal agent.
Final Word: Conclusion
To wrap up this cornerstone guide, we must return to the initial question: Can hallux rigidus be reversed? As we have explored through the lens of Dr. Mark Reynolds, the answer depends entirely on your definition of “reversal.” If you are looking for a biological reset to a 20-year-old joint, the answer is no. However, if you are looking for a Functional Reversal, where pain is absent, mobility is restored via footwear, and the “need” for surgery is eliminated, the answer for the vast majority of Grade 0-2 patients is a resounding yes.
The secret to success is not a “magic pill” or a single injection; it is the consistent application of mechanical offloading. By combining the right Best Walking Shoes for Hallux Rigidus with high-authority clinical staging, you move from a victim of a degenerative disease to an active manager of your own biomechanics.
Your 3-Step Reversal Plan
Stiffen Up: Buy Rocker-Bottom shoes today.
Offload: Add a Morton’s Extension.
Monitor: Check for “Rest Pain” monthly.
Frequently Asked Questions (Hallux Rigidus Reversal)
Can hallux rigidus go away on its own?
No. Because hallux rigidus is a structural degenerative condition involving cartilage loss and bone spur formation, it will not “heal” like a muscle strain. Without intervention, it typically progresses. However, with the “Reynolds Protocol” of stiff-soled shoes and orthotics, the symptoms can effectively disappear.
What is the fastest way to reverse big toe pain?
The fastest “symptomatic reversal” comes from switching to a rocker-bottom shoe and a custom Morton’s Extension. This immediately reduces the pressure on the MTP joint by up to 50%, often providing relief within 48 hours.
Is walking good for hallux rigidus?
Walking is excellent for overall health, but only if done in the correct footwear. Walking in flexible “minimalist” shoes or worn-out sneakers will accelerate the “grinding” of the joint. Always consult our guide on Shoes to Avoid with Hallux Rigidus before starting a new walking program.
At what point is surgery inevitable?
Surgery becomes inevitable when “Rest Pain” begins. It means your toe hurts even when you aren’t walking or when you can no longer perform daily activities despite using rocker-bottom shoes and orthotics for at least 6 months.
Can physical therapy reverse the “bump” on my toe?
No. Physical therapy is excellent for restoring the “Windlass Mechanism” and stretching the Achilles, which helps with Hallux Rigidus vs. Hallux Limitus. But it cannot dissolve a bone spur. PT “reverses” the stiffness of the soft tissue, but the bone spur remains a structural permanent fixture.
Is there a specific diet that reverses hallux rigidus?
While no diet “cures” arthritis, an anti-inflammatory protocol (Mediterranean style) can significantly reduce the perception of pain. By lowering systemic inflammation, a Grade 2 joint can feel as comfortable as a Grade 0. However, don’t be fooled by “miracle” supplements; diet is a management tool, not a structural fix.
Why does my big toe hurt more in the morning?
This is often due to stagnant inflammation. While you sleep, the inflammatory fluid settles in the joint space. As you take your first steps, the “jamming” begins immediately. This is a key indicator that you are moving from a functional to a structural stage, and you should review our Hallux Rigidus Stages and Grading guide.
Can I still wear high heels if I have hallux rigidus?
Generally, no. High heels force the MTP joint into maximum “extension,” which is the exact position that causes bone-on-bone grinding in hallux rigidus. If you must wear them, they must be a “platform” style with zero flex in the forefoot.
Does pulling on my toe (traction) help reverse the condition?
Manual traction can provide temporary relief by creating space in the joint, but it is not a permanent reversal. It’s like stretching a rubber band; once you let go, the joint returns to its compressed state. Consistent offloading via orthotics is the only way to maintain that “space” long-term.
How long do I have before Grade 2 becomes Grade 3?
This is the “Million Dollar Question.” Without intervention, the transition can happen in 2–5 years. However, with the “Reynolds Protocol” (rocker-bottom shoes and Morton’s extensions), many patients stay at Grade 2 for over a decade without further decay.


