
If you are researching hallux rigidus vs. hallux limitus, you are likely dealing with a frustrating “locking” sensation at the base of your big toe. While these two terms are often used interchangeably, in the world of clinical podiatry, they represent two very different points on a progressive timeline of big toe arthritis.
Understanding this distinction is the single most important factor in preserving your long-term mobility. Hallux limitus is the “warning stage,”، a functional restriction in which the joint remains healthy, and the condition is potentially reversible. Hallux rigidus, however, is the “destination,” a state of advanced arthritis where bone spurs and cartilage loss have made the joint permanently stiff.
In this definitive 2026 guide, we break down the biomechanics of both conditions and how identifying your specific status today can save you from a surgical fusion tomorrow.

Expert Vetted
Dr. Sarah Jenkins, DPM
Senior Orthopedic Podiatrist & Gait Analysis Specialist, HalluxRigidusCare
“Stiffness in the big toe isn’t just a foot issue; it’s a kinetic chain issue. If we don’t offload the MTP joint early, the knees and lower back pay the price within 18 months.”
What Is Hallux Limitus? (The “Functional” Warning Stage)
To understand hallux rigidus vs. hallux limitus, you must first understand that Hallux Limitus is a “mechanical” problem, not necessarily a “biological” one. In clinical podiatry, this is categorized as a Functional Blockage.
The Mechanics of the “Lock”
In a healthy foot, your big toe is the “engine” of your stride. As your heel lifts off the ground, your body weight rolls forward, and the big toe must bend upward (dorsiflex) between 40° and 60°. This allows for a smooth, efficient “toe-off.”
In hallux limitus, this motion is restricted, usually to 20–40°. While the toe is technically capable of moving, something is physically “jamming” the joint the moment you take a step.
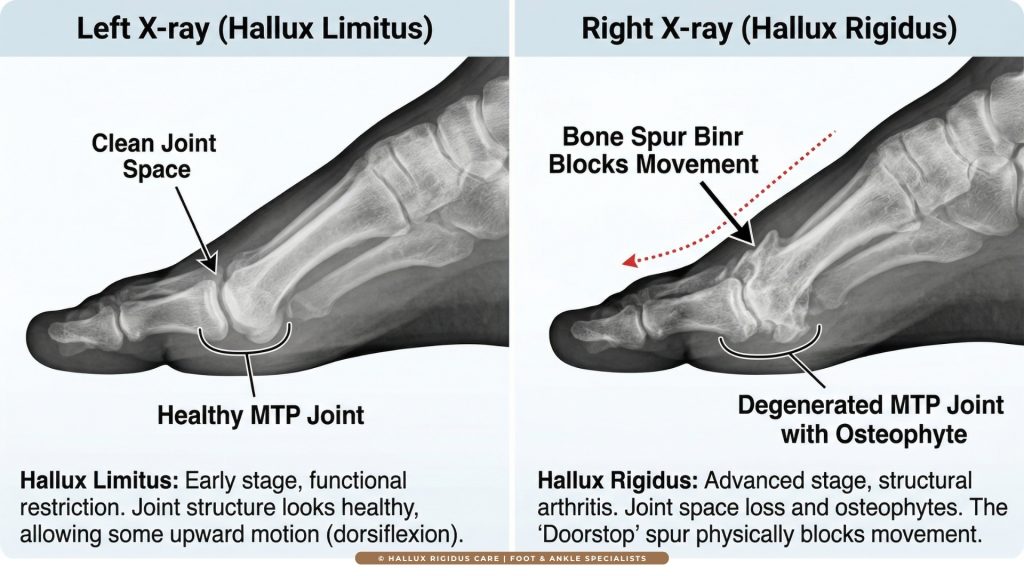
Why the X-Ray Looks Normal
The most frustrating aspect for patients in the limitus stage is that their X-ray often comes back “clean.” This is because, at this stage:
- The Cartilage is Intact: The smooth, slippery coating on the ends of your bones has not yet worn away.
- No “Bone-on-Bone”: There is still a healthy visible “gap” (joint space) between the metatarsal head and the toe bone.
- The Cause is Biomechanical: The restriction is usually driven by external factors such as a tight Achilles tendon or an “elevated first ray.”
The “Golden Window” for Reversal
Because there is no permanent structural decay, hallux limitus is often reversible. If you catch the condition in this stage, you are in the “Golden Window.” By using Custom Orthotics to “unlock” the joint, you can often restore a full range of motion and prevent the transition into permanent arthritis.
What Is Hallux Rigidus? (The “Structural” Destination)
If hallux limitus is a “mechanical jam,” hallux rigidus is a “broken engine.” This is the progressive, irreversible arthritic degeneration of the first MTP joint. The term literally translates from Latin as “Rigid Big Toe.”
The “Doorstop” Effect
Unlike the functional stage, hallux rigidus involves Structural Damage that is clearly visible on a weight-bearing X-ray. As the protective cartilage wears away, the bones begin to rub together. To protect itself, the body grows extra bone in the form of “Bone Spurs” (Osteophytes).
Did You Know?
The 1-in-40 Rule: Hallux rigidus is the most common form of arthritis in the foot. Statistically, 1 in every 40 adults over the age of 50 will develop this condition. Catching it in the ‘Limitus’ stage is the only way to avoid becoming part of that statistic.
These spurs typically form on the top (dorsal aspect) of the joint. They act exactly like a physical doorstop. No matter how much you stretch or exercise, the toe cannot bend upward because it is hitting a solid wall of bone.
Clinical Markers of Rigidus on X-ray:
- Joint Space Narrowing: The protective “gap” between your bones has disappeared or narrowed by more than 50%.
- Subchondral Sclerosis: The bone tissue appears “whiter” or denser on the X-ray, signaling that it is under extreme stress from friction.
- Subchondral Cysts: In advanced stages, small fluid-filled holes appear in the bone as the internal structure begins to fail.
The Kinetic Chain Domino Effect (The “Supination Escape”)
One of the most critical reasons to understand the hallux rigidus vs. hallux limitus distinction is to prevent secondary injuries. When your big toe becomes restricted or rigid, your body subconsciously changes how you walk to avoid the sharp, pinching pain of “pushing off.”
In clinical podiatry, this is known as Gait Compensation.
The “Supination Escape” Mechanic
In a healthy gait, your weight should roll from the heel, through the arch, and “launch” off the big toe. When that launch point is blocked by a functional jam (limitus) or a bone spur (rigidus), your brain tells your foot to “roll outward” onto the pinky toe side. This is called Supination.
The Domino Effect on Your Body
This “escape” mechanic rarely comes without a cost. Because your foot is hitting the ground at an unnatural angle, it sends a shockwave of misalignment up your entire leg:
- The Ankle: Walking on the outside of your foot stretches the lateral ligaments, leading to chronic ankle instability and frequent “rolling” of the ankle.
- The Knee: The outward roll causes the tibia (shin bone) to rotate unnaturally. This travels to the knee, often manifesting as IT Band Syndrome or lateral patellar tracking issues.
- The Hip & Lower Back: To compensate for the loss of “push” from the toe, your hip flexors have to “pull” your leg forward. Over time, this leads to Hip Bursitis and lower back misalignment.
If you have been diagnosed with hallux rigidus vs. hallux limitus, your X-ray report is the definitive map of your future. To establish true authority on your condition, you must understand the specific radiographic markers clinicians use to “stage” your disease.
1. Joint Space Narrowing (JSN)
Cartilage is invisible on a standard X-ray. Doctors estimate your cartilage health by measuring the “gap” between the metatarsal head and the toe bone.
- Hallux Limitus: The gap is wide and even.
- Hallux Rigidus: The gap is narrowed by 50% (Grade 2) or completely obliterated (Grade 3–4).
2. Subchondral Sclerosis (The “Whitening”)
On an X-ray, healthy bone appears soft and grey. When a joint is under extreme mechanical stress, the bone becomes denser to protect itself. If your report mentions “increased subchondral sclerosis,” it is a definitive sign that your joint is no longer absorbing shock correctly.
3. Subchondral Cysts & Loose Bodies
As the condition reaches Grade 3 (Severe), the pressure becomes so intense that joint fluid is forced into the bone, creating small “cysts.” In some cases, small pieces of bone or cartilage break off and float inside the joint. These are called Loose Bodies, and they act like “sand in the gears,” causing the joint to “lock” unexpectedly.
Clinical Staging Matrix (Coughlin-Shurnas)
| Clinical Feature | Hallux Limitus (Functional) | Hallux Rigidus (Structural) |
|---|---|---|
| X-Ray Findings | ✓ Structurally Normal | ⚠️ Bone Spurs & Narrowing |
| Range of Motion | 20–40° (Restricted) | 0–30° (Severely Limited) |
| Cartilage Status | Intact and Healthy | Partially or Fully Worn Away |
| Visible Bump? | Usually No | Yes (Dorsal Osteophyte) |
| Reversibility | Potentially Reversible | Permanent Damage |
*Scroll horizontally to view full table on mobile devices.
2026 Treatment Protocols (Where the Paths Diverge)
The most critical practical difference between hallux rigidus vs. hallux limitus is the clinical outcome you can realistically expect. Because one is a functional “jam” and the other is a structural “decay,” your treatment plan must match your specific stage.
1. Treating Hallux Limitus (The Goal: Reversal)
Since there is no permanent structural damage, hallux limitus responds effectively to conservative care. The objective is to “unlock” the joint mechanics and prevent the transition into permanent arthritis.
- Manual Physical Therapy: A therapist uses “Joint Distraction” to pull the toe forward, creating space before mobilizing the joint to restore the natural “glide.”
- Custom Orthotics: A prescription orthotic with a Morton’s Extension (a rigid plate under the big toe) is the gold standard. It prevents the toe from hitting its painful “jamming” point during your stride.
- Calf Stretching: Reducing tension in the Achilles tendon is vital. A tight calf “pulls” on the plantar fascia, which locks the big toe joint from below.
CLINICAL PRECAUTION
Never ignore a ‘dorsal bump’ forming on your big toe. This is not a bunion; it is a bone spur. Using standard orthotics without a specific Morton’s Extension can actually increase the pressure on the spur, worsening the inflammation.
2. Treating Hallux Rigidus (The Goal: Management & Preservation)
Once cartilage loss is visible on an X-ray, treatment shifts from “fixing” to “offloading.” We are now protecting a damaged engine from further wear.
- Rocker-Bottom Footwear: This is the #1 non-surgical intervention. Shoes like the HOKA Bondi or New Balance Fresh Foam More feature a curved sole. This sole performs the “roll” of the foot for you, eliminating the need for the MTP joint to bend.
- Injections: Cortisone or Hyaluronic Acid can reduce internal “grinding” inflammation for 3–6 months, providing a window for physical therapy.
- Surgical Intervention: If you reach Grade 3 or 4, surgery often becomes the only way to live pain-free:
- Cheilectomy: Shaving the “doorstop” bone spurs to restore motion (Ideal for Grade 1–2).
- Arthrodesis (Fusion): Permanently fusing the joint. This eliminates grinding pain forever and is the 2026 “Gold Standard” for Grade 4.
When managing hallux rigidus vs. hallux limitus, your lifestyle doesn’t have to end, but your equipment must change.
| Activity | With Hallux Limitus | With Hallux Rigidus |
|---|---|---|
| 👟 Running | Possible with Stiff-Sole Shoes | Difficult; Use Rocker-Soles |
| ⛰️ Hiking | Manageable; Stiff Shank Boots | Requires Poles + Rigid Boots |
| 🧘 Yoga | Avoid Deep Lunge Poses | Modify; Avoid Toe Flexion |
| 🚲 Cycling | Excellent; Low Impact | Gold Standard; Carbon Soles |
| 🏊 Swimming | Ideal; Zero Load | Ideal; Best Cardio Option |
Conclusion – Reclaiming Your Mobility in 2026
The hallux rigidus vs. hallux limitus distinction is a clinical roadmap. If you have been diagnosed with hallux limitus, you have a significant window of opportunity to act before permanent damage occurs. If your diagnosis is hallux rigidus, your focus must shift to Mechanical Offloading to save your larger joints from the kinetic chain domino effect.
“Hallux limitus is a biomechanical puzzle; Hallux rigidus is a structural decay. Solving the puzzle early is the only way to prevent the decay.”
— Sarah Jenkins, DPM, HalluxRigidusCare
Your 3-Step Strategy for Success:
- Stage Early: Get a weight-bearing X-ray to confirm if cartilage is intact.
- Immobilize: If you are Grade 2 or higher, switch to Stiff-Sole Footwear immediately.
- Consult: Discuss surgical options only after conservative “Mechanical Offloading” has been exhausted for at least 6 months.
Frequently Asked Questions About Hallux Rigidus vs. Hallux Limitus
1. Can hallux limitus be reversed without surgery?
Yes. Because hallux limitus is a “functional” restriction (Grade 0), the joint structure is still healthy. With targeted physical therapy to address the Windlass Mechanism, manual joint mobilization, and the use of Custom Orthotics with a Morton’s Extension. Many patients can “unlock” the joint and restore a full 40–60° range of motion, effectively reversing the condition before it becomes structural arthritis.
2. What is the main difference between Grade 2 and Grade 3 hallux rigidus?
The clinical distinction lies in Mid-Range Pain. In Grade 2 (Moderate), the pain primarily occurs at the “end-range” (when you bend the toe as far as it can go). In Grade 3 (Severe), the cartilage loss is so extensive that the joint hurts throughout the entire arc of motion. On an X-ray, Grade 3 will show Subchondral Cysts, which are rarely seen in Grade 2.
3. Why does my hallux rigidus cause knee and hip pain?
This is known as the Kinetic Chain Domino Effect. Because your big toe won’t bend, you subconsciously roll your foot outward (Supination) to avoid “pushing off” the painful joint. This causes your leg to rotate unnaturally, leading to IT Band Syndrome, lateral knee pain, and even lower back misalignment. Addressing your hallux rigidus stages early can save your larger joints from secondary injury.
4. Are rocker-bottom shoes mandatory for all hallux rigidus stages?
While not mandatory for Grade 0 (Limitus), Rocker-Bottom Shoes are the most effective non-surgical treatment for Grades 2, 3, and 4. By creating a curved sole, the shoe performs the “roll” of the foot for you. This eliminates the need for the MTP joint to bend, which is essential when your range of motion is less than 10 degrees.
5. How does a tight Achilles tendon contribute to big toe stiffness?
A tight Achilles tendon causes Equinus, which limits ankle upward motion. To compensate, the foot overpronates, which “jams” the first MTP joint during the gait cycle. This is the primary driver of Functional Hallux Limitus. Stretching the calf muscles is often the first step in “unlocking” a stiff big toe.
6. Is a Cheilectomy successful for Grade 3 Hallux Rigidus?
A Cheilectomy (bone spur removal) has a 90% success rate for Grades 1 and 2. However, for Grade 3, the success rate drops to approximately 70% because the underlying cartilage is already destroyed. While it may provide 5–7 years of relief, many Grade 3 patients eventually require a First MTP Joint Fusion for permanent results.
7. What does “Joint Space Narrowing” mean on my X-ray report?
Joint space narrowing is the primary radiographic marker for arthritis. Since cartilage is invisible on X-rays, doctors look at the “gap” between the bones. As the cartilage wears away, the bones get closer together. “Substantial narrowing” is the definitive indicator that you have moved from Hallux Limitus to Moderate (Grade 2) Hallux Rigidus.
8. Does losing weight help slow the progression of big toe arthritis?
Absolutely. The big toe joint bears nearly double your body weight during the “push-off” phase of walking. Clinical studies show that losing just 10 pounds can remove up to 40 pounds of pressure from the MTP joint with every step. This reduction in Mechanical Loading is the most effective way to stay at a lower clinical grade for a longer period.
9. Can I still run with hallux rigidus or hallux limitus?
Running is possible but requires equipment changes. For Hallux Limitus, you need a stiff-soled shoe to prevent excessive jamming. For Hallux Rigidus, you must transition to a high-stack, rocker-sole shoe (like the HOKA Bondi) or use a carbon-fiber insert to prevent the joint from bending during the stride.
10. Is a Joint Replacement better than a Fusion for Grade 4?
In 2026, Arthrodesis (Fusion) remains the “Gold Standard” for Grade 4. While joint replacements (Arthroplasty) preserve some motion, they have a higher failure rate in the foot due to the extreme pressures involved. A fusion provides a permanent, stable, and pain-free solution that allows patients to return to hiking, cycling, and even light jogging.
- Best Insoles for Hallux Rigidus (2026): Carbon Fiber Plates, Morton’s Extensions & Orthotics Compared - July 28, 2026
- Best Rocker Bottom Shoes for Hallux Rigidus (2026): 5 Picks That Change How You Walk - April 21, 2026
- Best Cycling Shoes for Hallux Rigidus (2026): 5 Top Stiff-Sole Picks for Road & MTB - April 1, 2026


