
If you have been diagnosed with big toe arthritis, you have likely heard the terms “Hallux Limitus” and “Hallux Rigidus” used interchangeably. However, in the world of clinical podiatry, these represent very different points on a progressive timeline. Understanding the stages of hallux rigidus is the single most important factor in preserving your long-term mobility.
Hallux Rigidus affects approximately 1 in 40 adults over the age of 50, making it the most common arthritic condition of the foot. Despite its prevalence, over 60% of patients are not properly staged at their first podiatry visit. They are delaying the most effective, grade-specific treatments by months or even years.
The Coughlin-Shurnas Grading System: The Gold Standard for Big Toe Arthritis
The “stage” of your condition, classified by the globally recognized Coughlin-Shurnas Grading System, is the primary metric that specialists use to determine your prognosis. Are you a candidate for custom orthotics, or has the joint decayed to the point where a total joint fusion is the only way to live pain-free?
Below is the 2026 Clinical Staging Matrix, summarizing the progression from functional stiffness to structural rigidity:
| Grade | Clinical Severity | Dorsiflexion (ROM) | X-Ray Evidence | Primary Symptom |
|---|---|---|---|---|
| Grade 0 | Pre-Arthritis | 40–60° (Normal) | Structurally Normal | Morning stiffness; mild aching |
| Grade 1 | Mild | 30–40° | Small dorsal bone spur | Pain during the “push-off” phase |
| Grade 2 | Moderate | 10–30° | 50% Joint space loss | Bony bump; pain with stairs |
| Grade 3 | Severe | <10° | Subchondral cysts present | Constant pain; visible limping |
| Grade 4 | End-Stage | ~0° (Frozen) | Bone-on-bone grinding | Pain at rest; total rigidity |
Source: Based on the Coughlin-Shurnas Classification (2026 Clinical Guidelines)
The Anatomy of a Stiff Big Toe: Understanding the First MTP Joint “Engine”
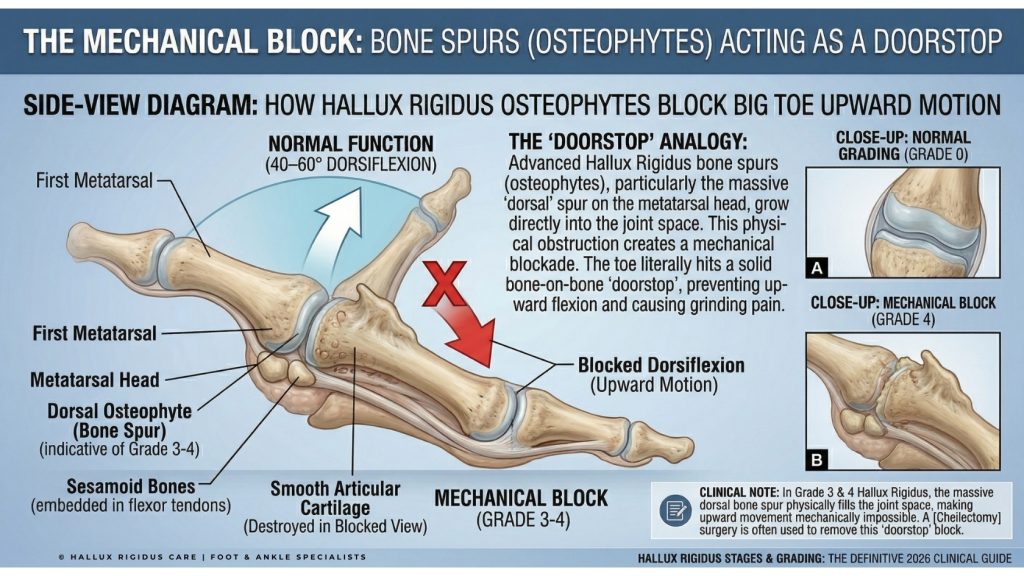
To understand the grading system, we must first look at the anatomy of the First Metatarsophalangeal (MTP) Joint. This joint is the “engine” of the human gait. Every time you take a step, your body weight rolls over this joint. To do this efficiently, the big toe must achieve a minimum of 40–60° of dorsiflexion
In a healthy joint, the ends of the bones are covered in smooth, slippery articular cartilage. This allows the bones to glide over one another without friction. Hallux Rigidus (Latin for “Stiff Big Toe”) occurs when this cartilage wears away.
As the protective cushion disappears, the body attempts to stabilize the failing joint by growing extra bone. These “bone spurs,” or osteophytes, typically form on the top (dorsal aspect) of the joint, acting like a physical doorstop that prevents the toe from bending.
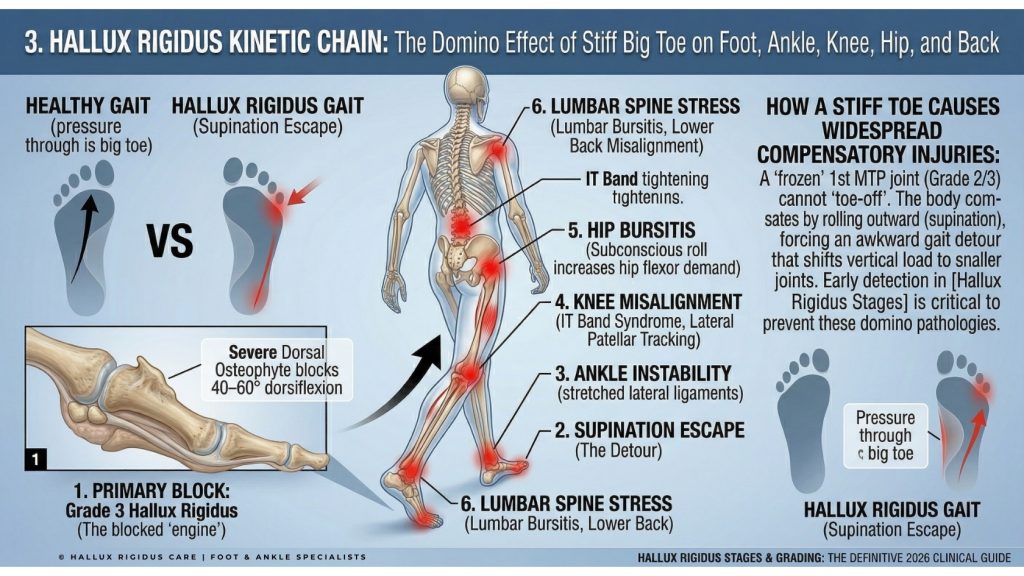
The Kinetic Chain: How Hallux Rigidus Stages Cause Knee, Hip, and Back Pain
One of the most critical reasons to monitor your hallux rigidus stages is to prevent secondary injuries. When your big toe becomes rigid, your body subconsciously changes how you walk to avoid the pain of “pushing off.” This is known as Gait Compensation.
Instead of rolling over the big toe, patients often “roll” to the outside of their foot (supination). According to the American Orthopaedic Foot & Ankle Society (AOFAS), this altered mechanics puts abnormal stress on the:
- Ankle: Leading to chronic lateral ankle instability.
- Knee: Causing the patella (kneecap) to track incorrectly.
- Hip & Lower Back: Forcing the hip flexors to “pull” the leg forward rather than allowing the foot to “push” it.
If you are experiencing knee, hip, or lower back pain alongside toe stiffness, do not treat these joints in isolation. Without addressing the root mechanical failure at the first MTP joint, secondary joint treatments will provide only temporary relief. Always request a comprehensive kinetic chain biomechanical assessment before pursuing any knee or hip intervention.
5 Hallux Rigidus Stages: From Early Stiffness to Total Rigidity
To accurately stage your hallux rigidus, clinicians use the Coughlin-Shurnas scale. This five-point system is the global standard because it doesn’t just look at an X-ray; it looks at how the joint functions in your daily life.
Below is the clinical breakdown of each grade, including the 2026 “Gold Standard” treatments for each.
Grade 0 Hallux Rigidus: Functional Hallux Limitus (The Pre-Arthritis Warning Stage)
Grade 0 is the most elusive of the hallux rigidus stages. At this point, the joint is structurally healthy, but it is “functionally” restricted. This stage is technically referred to as Hallux Limitus.
- Radiographic Findings (X-Ray): The X-ray will appear entirely normal. There is no joint space narrowing, and no bone spurs (osteophytes) are visible.
- Clinical Symptoms: You likely feel a “tightness” or a dull ache at the base of the big toe after a long day of walking or standing. You may notice that the joint feels stiff first thing in the morning, but “loosens up” after a few minutes of movement.
- Range of Motion (ROM): Your upward bend (dorsiflexion) is still within the normal range of 40–60°, but it may feel restricted at the very end of the movement.
- 2026 Treatment Strategy: This is the only stage where the condition is potentially reversible. Since no structural damage has occurred, the goal is to “unlock” the joint.
- Physical Therapy: Manual mobilization of the first MTP joint.
- Calf Stretching: Reducing tension in the Achilles tendon, which often drives big toe stiffness.
- Footwear: Transitioning to the best walking shoes for Hallux Rigidus to prevent the joint from “grinding” into the next stage.
This is the only stage where full reversal is clinically achievable. Unlike Grades 1–4, where structural damage is permanent, Grade 0 involves no cartilage loss. A targeted 8–12 week physical therapy program combined with proper footwear has been shown to restore full joint function in the majority of patients. Do not miss this critical window!
Grade 1 Hallux Rigidus: Mild Structural Decay (The Onset of Bone Spurs)
In Grade 1, the condition moves from a functional “tightness” to a structural “disease.” This is the first stage where a radiologist can see the arthritis beginning to form.
- Radiographic Findings (X-Ray): You will see the earliest signs of a Dorsal Osteophyte (a small bone spur on top of the joint). The metatarsal head may appear slightly flattened, and there is a subtle “whitening” of the bone known as subchondral sclerosis, indicating the bone is under increased stress.
- Clinical Symptoms: Pain is no longer just a “dull ache.” It becomes a sharp, pinching sensation specifically during the “push-off” phase of your stride. You may notice slight swelling around the joint after a workout.
- Range of Motion (ROM): Dorsiflexion is now limited to 30–40°.
- 2026 Treatment Strategy: The priority is “Mechanical Offloading.”
- Custom Orthotics: A prescription orthotic with a Morton’s Extension (a rigid plate under the big toe) is the gold standard. It prevents the toe from hitting that painful 30° limit.
- Activity Modification: If you are a runner, this is the time to integrate Stiff-Sole Cycling Shoes to maintain cardio without joint wear.
Grade 2 Hallux Rigidus: Moderate Arthritis (The Clinical Tipping Point)
Grade 2 is the most common stage for initial diagnosis because the pain is finally high enough to disrupt daily life. This is when the famous “bony bump” on top of the toe becomes prominent.
- Radiographic Findings (X-Ray): X-rays now clearly show Joint Space Narrowing. This means the protective cartilage has worn down by 50% or more. Bone spurs are now “moderate to large” and may appear on the top, medial, and lateral sides of the joint.
- Clinical Symptoms: You likely have difficulty fitting into standard dress shoes or slim sneakers. Walking on uneven ground (like grass or sand) becomes very painful. The joint may feel warm to the touch due to chronic inflammation.
- Range of Motion (ROM): Dorsiflexion is significantly reduced to 10–30°.
- 2026 Treatment Strategy: Conservative care is still the first line, but surgery enters the conversation.
- Footwear: Rocker-bottom shoes (like HOKA Bondi) become a daily necessity.
- Cheilectomy Surgery: This is the “Golden Window” for a Cheilectomy. By surgically removing the “doorstop” bone spurs, a surgeon can often restore enough motion to return a patient to a Grade 1 lifestyle.
Grade 2 represents the “Goldilocks Zone” for surgical intervention. The bone spurs are large enough to cause significant pain, yet the underlying cartilage retains enough integrity for a joint-preserving procedure. Research shows a 90%+ patient satisfaction rate for Cheilectomy at Grade 2, versus 70–75% at Grade 3. Once Grade 3 is reached, the first MTP fusion becomes increasingly likely as the final outcome.
Grade 3 Hallux Rigidus: Severe Joint Damage (Advanced Cartilage Loss)
At Grade 3, the joint has sustained substantial, irreversible damage. The “cushion” between the bones is nearly gone.
- Radiographic Findings (X-Ray): The joint space is “severely narrowed” or “obliterated.” You will see Subchondral Cysts (fluid-filled holes in the bone) and significant bone-on-bone contact. Osteophytes now encircle the entire joint.
- Clinical Symptoms: Pain occurs during mid-range motion, not just when you bend the toe up. You likely walk with a limp or roll onto the outside of your foot (supination) to avoid using the big toe entirely. This often leads to secondary knee and hip pain.
- Range of Motion (ROM): Dorsiflexion is less than 10°.
- 2026 Treatment Strategy: * Moberg Osteotomy: A procedure that realigns the toe bone to give you more “usable” upward movement.
- Interpositional Arthroplasty: Using a small tissue “spacer” to prevent bone-on-bone grinding while preserving some motion.
Grade 4 Hallux Rigidus: End-Stage Arthritis (Ankylosis)
Grade 4 is the final stage of hallux rigidus. The joint is essentially “fused” by a combination of massive bone spurs and scar tissue.
- Radiographic Findings (X-Ray): Complete loss of the joint space. The two bones may appear to be “merging” into one. Total joint destruction is evident.
- Clinical Symptoms: Pain at rest. Even when you aren’t walking, the toe may throb. Crucially, it now hurts to bend the toe down (plantarflexion) as much as it hurts to bend it up. This “global pain” is the hallmark of Grade 4.
- Range of Motion (ROM): Functionally 0°. The toe is “frozen.”
- 2026 Treatment Strategy: * First MTP Joint Fusion (Arthrodesis): This is the Gold Standard for Grade 4. By permanently fusing the joint in a slightly upward position, the surgeon eliminates the grinding pain forever. Most patients can return to hiking, cycling, and even light jogging after a successful fusion.
Decoding Your X-Ray Report: Identifying Key Radiographic Markers
One of the most dangerous aspects of progressing through the hallux rigidus stages is not the toe pain itself, but the “Domino Effect” it has on the rest of your body. In clinical podiatry, this is known as Gait Compensation.
When your big toe loses its ability to dorsiflex (bend upward), your body is forced to find a “detour” to move you forward. This detour rarely comes without a cost to your other joints.
The “Supination Escape” Mechanic: Why Your Foot Rolls Outward
In a healthy gait, your weight should roll from the heel, through the arch, and “launch” off the big toe. When you reach Grade 2 or 3 Hallux Rigidus, that launch point is blocked by bone spurs. To avoid the sharp “bone-on-bone” pain, your brain subconsciously tells your foot to “roll outward” onto the pinky toe side. This is called Supination.
2026 Clinical Recovery Milestones: What to Expect After Surgery
If you have been diagnosed with Grade 2 or higher, you may already be experiencing these secondary issues:
- Metatarsalgia of the Lesser Toes: Because the big toe isn’t carrying its 40% share of the load, the 2nd and 3rd toes take the brunt. This leads to “stress fractures” and painful calluses under the ball of the foot.
- Ankle Instability: Walking on the outside of your foot stretches the lateral ligaments, making you more prone to “rolling your ankle.”
- Knee and Hip Misalignment: The outward roll of the foot causes the tibia (shin bone) to rotate unnaturally. This travels up the kinetic chain, often manifesting as IT Band Syndrome or Lateral Hip Bursitis.
Decoding Your X-Ray Report: Identifying Key Radiographic Markers at Each Stage
Most patients receive an X-ray report filled with “Medical Latin” that is difficult to decipher. To establish Topical Authority, we must break down the specific radiographic markers that determine your Coughlin-Shurnas grade.
Subchondral Sclerosis: What the “Whitening” of Your Bone Means on X-ray
On an X-ray, bone appears white and soft tissue appears black. When a joint is under extreme mechanical stress, typical in Grade 1 and 2 Hallux Rigidus, the bone becomes denser to protect itself. This is called Sclerosis. If your report mentions “increased subchondral sclerosis,” it is a definitive sign that your joint is no longer absorbing shock correctly.
Joint Space Narrowing: The Ultimate Metric for Assessing Cartilage Health
Cartilage is invisible on a standard X-ray. Doctors estimate your cartilage health by measuring the “gap” between the metatarsal head and the phalanx.
- Mild Narrowing: Grade 1.
- Moderate Narrowing (>50% loss): Grade 2.
- Obliterated Joint Space: Grade 3 or 4.
Subchondral Cysts and Loose Bodies: Red Flags for Severe Disease (Grades 3–4)
As the condition reaches Grade 3 Severe Hallux Rigidus, the pressure becomes so intense that joint fluid is forced into the bone, creating small “cysts” or “geodes.” If your X-ray report mentions “cystic changes,” it is a clinical red flag that the structural integrity of the bone is at risk, often making Arthrodesis (Fusion) a more viable long-term option than a simple bone spur removal.
In advanced stages, small pieces of bone or cartilage can break off and float inside the joint capsule. These are called Loose Bodies. They act like “sand in the gears,” causing the joint to “lock” or “catch” unexpectedly. This is a primary symptom that differentiates Grade 3 from Grade 4, as Grade 4 joints are usually too tight for loose bodies to move freely.
Conclusion: Reclaiming Your Mobility in 2026
The hallux rigidus stages are not a sentence of disability; they are a clinical roadmap. By identifying whether you are dealing with early-stage stiffness or end-stage rigidity, you can stop guessing and start implementing the right mechanical solutions.
The 2026 Strategy for Success:
- Stage Early: Get a weight-bearing X-ray to determine your Coughlin-Shurnas Grade.
- Immobilize: If you are Grade 2 or higher, switch to Stiff-Sole Footwear immediately.
- Consult: Discuss surgical options like Cheilectomy or Fusion only once conservative “Mechanical Offloading” has been exhausted.
Frequently Asked Questions About Hallux Rigidus Stages and Grading
1. Can Grade 2 Hallux Rigidus be reversed without surgery?
No. Once a dorsal osteophyte (bone spur) has formed and cartilage has been lost, the structural damage is permanent. However, you can effectively “reverse” the symptoms. By using Custom Orthotics with a Morton’s Extension and Stiff-Sole Rocker Shoes, you can bypass the damaged joint area, allowing you to walk pain-free as if you were still at Grade 0 or 1.
2. What is the main difference between Grade 2 and Grade 3 Hallux Rigidus?
The clinical distinction lies in Mid-Range Pain. In Grade 2, the pain primarily occurs at the “end-range” (when you bend the toe as far as possible). In Grade 3 Severe Hallux Rigidus, the cartilage loss is so extensive that the joint hurts throughout the entire arc of motion. On an X-ray, Grade 3 will show “Subchondral Cysts,” which are rarely seen in Grade 2.
3. Why is Grade 0 called “Functional Hallux Limitus”?
It is called “functional” because the joint itself is still healthy on an X-ray, but the function is restricted. Usually, a tight Achilles tendon or an elevated first metatarsal bone prevents the joint from sliding properly. If caught at Grade 0, the progression to structural arthritis can often be stopped entirely through targeted physical therapy.
4. Is a Cheilectomy successful for Grade 3 Hallux Rigidus?
A Cheilectomy (bone spur removal) has a 90% success rate for Grades 1 and 2. For Grade 3, the success rate drops to approximately 70-75% because the underlying cartilage is already significantly damaged. While it may provide 5–7 years of relief, many Grade 3 patients eventually require a First MTP Joint Fusion for permanent results.
5. Can Hallux Rigidus cause knee or hip pain?
Yes. This is known as Kinetic Chain Compensation. Because your big toe won’t bend, you subconsciously roll your foot outward (supination). This causes your leg to rotate unnaturally, leading to IT Band Syndrome, lateral knee pain, and even lower back misalignment. Addressing your hallux rigidus stages early can save your larger joints from secondary injury.
6. What does “Joint Space Narrowing” mean on my X-ray report?
Joint space narrowing is the primary radiographic marker for arthritis. Since cartilage is invisible on X-rays, doctors look at the “gap” between the bones. As the cartilage wears away, the bones get closer together. “Substantial narrowing” is the definitive indicator that you have moved from Mild (Grade 1) to Moderate (Grade 2) Hallux Rigidus.
7. Are “Rocker Bottom” shoes mandatory for Grades 3 and 4?
For Stage 3 and 4 Hallux Rigidus, rocker-bottom shoes are the most effective non-surgical treatment. By creating a curved sole, the shoe performs the “roll” of the foot for you. This eliminates the need for the MTP joint to bend, which is essential when your range of motion is less than 10 degrees.
8. Does losing weight help slow the progression of Hallux Rigidus?
Absolutely. The big toe joint bears nearly double your body weight during the push-off phase of walking. According to clinical studies, losing just 10 pounds can remove up to 40 pounds of pressure from the joint with every step. This reduction in “Mechanical Loading” is the most effective way to stay at Grade 1 or 2 for a longer period.
9. Why is my big toe arthritis more painful in the winter?
Cold weather causes joint fluid (synovial fluid) to become thicker and less lubricating. Additionally, barometric pressure changes can cause the bone tissue to expand slightly, which increases the “grinding” sensation in the Grade 2 and 3 stages. Using Infrared Toe Warmers can help manage this seasonal stiffness.
10. Is a Joint Replacement better than a Fusion for Grade 4?
In 2026, Arthrodesis (Fusion) remains the “Gold Standard” for Grade 4. While joint replacements (arthroplasty) preserve some motion, they have a higher failure rate in the foot due to the extreme pressures involved. A fusion provides a permanent, stable, and pain-free solution that allows patients to return to hiking, cycling, and active lifestyles.
- Best Insoles for Hallux Rigidus (2026): Carbon Fiber Plates, Morton’s Extensions & Orthotics Compared - July 28, 2026
- Best Rocker Bottom Shoes for Hallux Rigidus (2026): 5 Picks That Change How You Walk - April 21, 2026
- Best Cycling Shoes for Hallux Rigidus (2026): 5 Top Stiff-Sole Picks for Road & MTB - April 1, 2026


